Preventing child mortality through the enhancement of integrated community-based programmes for under-five malnutrition management: results from the Rainbow Project study in Zambia
Stefania Moramarco,1,2 Giulia Amerio,2 Ersilia Buonomo1
1 Department of Biomedicine and Prevention, University of Rome Tor Vergata
2 Rainbow Project/Association Pope John 23rd in Zambia, Associazione Papa Giovanni XXIII
Introduction
Worldwide, more than 50 million children under the age of five years are estimated to be still affected by general acute malnutrition, with 16 million having Severe Acute Malnutrition (SAM) and a further 33 million having Moderate Acute Malnutrition (MAM).1 General acute malnutrition, when untreated, is attributable to the 12.6% of the 6.9 million deaths among under-five children.2 Most of these children live in South Asia and Sub-Saharan Africa, being 15 times more likely to die before the age of 5 than children in high income countries.3 The community-based management of acute malnutrition (CMAM), which evolved from the Community-Based Therapeutic Care (CTC) approach developed in 2001 with all its components – Inpatient Therapeutic Care (ITC), Out-patient Therapeutic Program (OTP), Supplementary Feeding Program (SFP), community engagement – is unequivocally advocated as an effective programme to address acute malnutrition for children aged 6 to 59 months.4,5,6 Actually globally implemented in more than 70 countries,7 the main aim of the CMAM programme is to reduce child mortality and morbidity by providing effective treatment of acute malnutrition, thanks to the community early identification and timely management. However, the coverage of all its components is still far to be reached at large scale in low-middle income settings. In fact, it can happen that local governments do not have sufficient capacity to integrate all the CMAM components as a routine national health care service. As a result, the programmes for Moderate Acute Malnutrition-MAM (i.e SFPs) and Severe Acute Malnutrition-SAM (i.e. OTPs) risk to stay linked only when the same body supports both activities. International agencies and Non-Governmental Organizations (NGOs) often provide systematic help to local governments for the CMAM activities through a combination of technical support, provision of resources, logistic, trainings, supervision, monitoring and evaluation activities. In particular, when lack of local resources occurs, the programmes for the MAM management are likely to be separated from the governmental services, being run directly from UN agencies or NGOs. With specific regard to Zambia, the reduction of child malnutrition is still a national public health priority. Unfortunately, the CMAM main components in Zambia are not fully implemented or integrated at a large scale in the local health system. To offer a response to the fight of child malnutrition in the Ndola district, the non-governmental organization Rainbow Project, under the Association Pope John 23rd, is running SFPs since more than twenty years, supporting the local health system in the community management of child malnutrition. The Rainbow SFPs are well-known and well-implemented in the field, providing a full package of nutrition-sensitive and nutrition-specific activities, in order to allow mothers/guardians to acquire basic nutrition skills and child health knowledge.8 All these activities are coupled by continuous monitoring and evaluation, close supervision, strong collaboration and network with the local health authorities. The community engagement is a paramount component of Rainbow model, as expected in the CMAM, since it allows early case-detection of malnourished children at community level, increasing coverage of services and positively impacting on health outcomes.
The Rainbow Project Study
A doctoral research (in Nursing Sciences and Public Health, University of Rome Tor Vergata) was carried out (years 2015-2017) to report the long field-based experience of Rainbow SFPs in Zambia (Ndola District). The main objective was to assess programme’s effectiveness as an integrated model of surveillance, treatment and prevention of child malnutrition in the specific local context.
During the first year of PhD, the Rainbow model was described, assessed and evaluated. The first research study was conducted between 2012 and 2014 on a sample of 858 malnourished children (either with MAM, SAM or underweight) admitted to the SFPs.9 The aim was to assess the programme’s outcomes, identifying main strengths and areas for improvement. The SFPs showed to be already effective in the general management of child malnutrition, with optimum results especially for MAM children (the specific target of SFPs): 86.1% was the recovery rate compared to >75% threshold prescribed in the international Sphere Standards; 2.8% was the death rate compared to <3% SFP acceptability.10 Mortality rates exceeded international standards when considering the SAM sample (12.4% compared to <10% acceptability), which mainly affected even the overall sample mortality: 5.6% for MAM, SAM and underweight analysed together. HIV infection, SAM and very low weight-for-age (WAZ <-3 SD) at admission were found as main predictors of mortality (HR: 3.1; HR: 3.8; and HR: 3.1 respectively). These results suggested the need for improvements: the adequacy of the food supplement distributed was specifically investigated, since even the average weight gain was slightly below the UNHCR/WFP standards of 3g/kg/die.11 As new proposal, the amount of the specific food supplement distributed (high energy protein supplement - HEPS) was increased.
Therefore, the second year of PhD research, was mainly dedicated to promote implementations at field levels. The food schedule was revised and operators of the SFPs trained to conduct the nutritional counseling accordingly.12 The quality of HEPS recipe was improved by suggesting to add sugar and oil (both of which ingredients were provided by the project) during the porridge preparation. With specific regard to HIV, the community volunteers’ knowledge on Voluntary Counseling and Testing (VCT) was strengthened, by continuous training and workshop run in close collaboration with the District Health Management Teams (DHMT). The counseling activities were always conducted in private environment, with full respect of people privacy.
After filling the gaps in activities, the performance of Rainbow SFPs was reassessed in 2015–2017, the third year of PhD research. Data for 900 under-five years old malnourished children were analysed for the second study.13 Rainbow SFPs confirmed their effectiveness in MAM management, now with better performances showed even in the main areas previously identified as critical. General improvements in all rates of main indicators, meeting the international targets of reference (Sphere, UNHCR/WFP), were noted when comparing to the previous programmes’ outcomes. Halving the child mortality rates was the main goal achieved: when considering the overall sample, the death rate had a peak down, decreasing from 5.6% to 3.1%, p = 0.01.
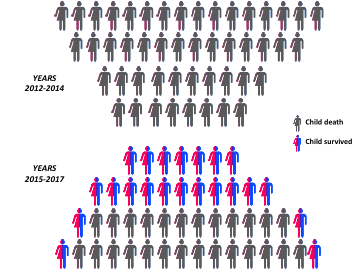
Figure 1 portrays the number of children dying in SFPs in 2012-14 compared with that of 2015-17. The figure shows the gain in children lives achieved during the second programmes’ evaluations, after enhancing the programmes’ activities, with almost half more children recovered from malnutrition.
Figure 1 - Additional children’ lives saved after enhancing the nutritional programmes.
As direct consequence of mortality reduction, the recovery rate increased (from 82.6% to 85.7%), while the defaulting slightly decreased (11.8% vs 11.2%).
Impressive results were also provided for SAM children: the mortality rate was halved from 12.4% to 6.7%, p = 0.006. This is an important result since shows that, when other targeted nutritional interventions are disrupted, SFPs could be effective in supporting the management of the severest cases. As a novel aspect of the community-based management of child malnutrition, Rainbow SFPs have been effective even in the nutritional rehabilitation of children underweight. In fact, although International guidelines do not provide specific targets for those children, outcomes fully met the available indicators: 85.9% recovered; 13.8% defaulters; 0.3% deaths. A statistically significant increase in the average weight gain (p < 0.001) was noted after the redoubling of HEPS that allowed also a reduction in the mean length of stay for recovered children, as proposed in the previous study. However, the daily gains in mean grams per weight was still below the international target, but in line with reviews of the literature for programmes using blended flour (2 g/kg/day).14 Sharing food within the household could have been a potential explanation for the quite poor mean weight gain.
HIV infection (HR 5.5; 1.9–15.9 CI), WAZ <–3 (HR 4.6; 1.3–16.1 CI), and kwashiorkor (HR 3.5; 1.2–9.5 CI) still remained the major predictors of mortality. These results supported the choice to admit to the programme different forms of acute malnutrition (SAM, underweight) other than MAM, in order to not leave out children most in need of nutritional rehabilitation when CMAM is not fully implemented. The targeted trainings for community volunteers on voluntary counseling and testing (VCT) conducted during the years of implementation showed their effectiveness: the integration of HIV/AIDS counseling as a main activity of the nutritional programmes consistently increased the guardians’ awareness of children’s HIV status: 30% more diagnosis (p<0.001) than in 2012-14 were achieved, with only the 8% of children still remaining with an HIV status unknown at time of discharge from SFPs. Despite the great result obtained, this last finding underscores that stigma of HIV and fear of discrimination still exist in Zambia.
Further researches on ongoing activities and implementations need to continue for maintaining high performance and standards of the existing programmes, in order to tackle child malnutrition in an area at high prevalence of HIV/AIDS, malaria and tuberculosis.15 In addition, we don’t have to forget that other indicators of malnutrition, such as growth velocity16 and motor milestones development,17 could play an important role for optimizing the holistic care of malnourished children.
Lesson learned
Academia are incubators of knowledge and innovation that can be channeled towards efforts to achieve Zero Hunger.18 This doctoral research in Zambia provides lessons to other countries and consistent evidence-based results: community-based programmes already existing at field level are fully effective in malnutrition management and more especially in preventing children deaths. More specifically, the Rainbow model in Zambia, which integrated child malnutrition treatment and prevention, showed its effectiveness in acting as major public health programmes for health prevention and care of children in food insecurity and HIV endemic contexts. Our results demonstrate that well-trained community volunteers and local staff, when accurately supervised and strong monitored, are capable not only to identify and manage cases of malnutrition, but also to provide accurate, reliable and trustable data. During the three years PhD research, monitoring and evaluation activities became more systematic and punctual, involving also the academic participation. This answers to the most recent FAO call (World Food Day 2018) for strategic partnerships with academia and research institutions, in order to generate significant and relevant information to address the challenges posed by hunger and malnutrition.
From our experience, monitoring and evaluation activities, routine assessment, technical support and advice included as leading practices, form the basis for the evaluation of programmes’ effectiveness. All those activities have allowed early identification of critical areas and have provided a solid evidence-base to inform decision-making. The Rainbow programme has quickly adapted and evolved over the years to the specific local scenario, by tailoring technical assistance and training to respond to identified gaps. Adjustments resulted in significant enhancement of its general performance.
Currently, nearly 1,900,000 children under-five years of age are living in Zambia,19 with 6% of them still being affected by general acute malnutrition20 (nearly 114,000). If not timely treated, they are at high risk of dying soon. SFPs as Rainbow Project, when well integrated in the CMAM and appropriately run, hold an important role as safety net for those children. Our findings feed the evidence that investing in community nutritional programmes, at a successfully recovery rate of 85% with less than 3% death rate, can successfully support Zambian health services in the management of child malnutrition, saving thousands of children lives.
Conclusion
Childhood malnutrition rates remain alarming, being a major public health problem throughout the developing world. Nearly half of the related death could be prevented by treating the nutritional status of children. When CMAM is not fully covered or scaled-up in all its components by local health authorities, nutritional programmes already existing and implemented in the field, usually run by NGOs, hold a great potential for cooperating to children treatment and care, not neglecting any form of child malnutrition. Monitoring and evaluation are essential tools especially in limited resource settings to demonstrate reliability of the organisations and effectiveness of the programmes, to drive changes that might lead to more improved health outcomes, and to efficiently allocate money to the most effective approaches. Identification of main gaps in programmes’ performance, with targeted and sustainable changes made accordingly, even when they seem small, can have high impact on programmes’ outcomes, therefore saving even more children lives.
References
- No Wasted Lives Initiative: The State of Severe Malnutrition Website. Available online: http://www.severemalnutrition.org/en/home/Ge
- Black RE, Victora, CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. et al. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451.
- UNICEF website. Children: Reducing Mortality. 19 September 2018. https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality
- WHO, UNICEF, WF, UN System Standing Committee on Nutrition. Community-Based Management of Severe Acute Malnutrition. A Joint Statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children’s Fund. Available online: http://www.who.int/nutrition/topics/Statement_community_based_man_sev_acute_mal_eng.pdf
- World Health Organization. Management of Severe Malnutrition: A Manual for Physicians and Other Senior Health Workers. Geneva 1999. Available online: http://whqlibdoc.who.int/hq/1999/a57361.pdf
- Valid International. Community-Based Therapeutic Care (CTC): A Field Manual. Available online: http://www.concernusa.org/content/uploads/2015/08/ctc_manual_v1_oct06.pdf
- Food and Nutrition Technical Assistance III Project (FANTA). 2018. Training Guide for Community-Based Management of Acute Malnutrition (CMAM). Washington, DC: FHI 360/FANTA.
- Moramarco S, Amerio G, Gozza Maradini G, Garuti E. Rainbow Project: A Model to Fight Child Malnutrition in Zambia. In Turning Rapid Growth into Meaningful Growth: Sustaining the Commitment to Nutrition in Zambia; Harris, J., Haddad, L., Grütz, S.S., Eds.; Institute of Development Studies: Brighton, UK, 2014; pp. 57–61. Available online: https://opendocs.ids.ac.uk/opendocs/bitstream/handle/123456789/4463/Zambia%20Special%20Collection%20full%20version.pdf
- Moramarco S, Amerio G, Ciarlantini C, Kasengele Chipoma J, Kakungu Simpungwe M, Nielsen-Saines K, Palombi L, Buonomo E. (2016). Community-Based Management of Child Malnutrition in Zambia: HIV/AIDS Infection and Other Risk Factors on Child Survival. Int. J. Environ. Res. Public Health.
- The SPHERE Project. (2011). The Sphere Handbook: Humanitarian Charter and Minimum Standards in Disaster Response, 3rd ed.; The SPHERE Project: Geneva, Switzerland.
- UNHCR/WFP. (2011). Guidelines for Selective Feeding: The Management of Malnutrition in Emergencies.
- Moramarco S, Amerio G, Chafula Muyaba L, Bonvecchio D, Abramo E, Palombi L, et al. Nutritional Counseling Improves Dietary Diversity and Feeding Habits of Zambian Malnourished Children Admitted in Rainbow Nutritional Programs. Biomedicine & Prevention; 2017.
- Moramarco S, Amerio G, Kasengele Chipoma J, Nielsen-Saines K, Palombi L, Buonomo E (2018). Filling the Gaps for Enhancing the Effectiveness of Community-Based Programs Combining Treatment and Prevention of Child Malnutrition: Results from the Rainbow Project 2015–17 in Zambia. Int. J. Environ. Res. Public Health.
- Matilsky DK, Maleta K, Castleman T, Manary MJ. Supplementary Feeding with Fortified Spreads Results in Higher Recovery Rates Than with a Corn/Soy Blend in Moderately Wasted Children. J. Nutr. 2009, 139, 773–778
- Palombi L, Moramarco S. Health in Sub-Saharan Africa: HIV, TB and Malaria Epidemiology. In Multidisciplinary Teleconsultation in Developing Countries edited by Bartolo M, Ferrari F. Springer International Publishing - Springer Nature 2018.
- Buonomo E, Germano P, Moramarco S. Rossi R, Malizia A, Scarcella P, et al. Early Assessment of Weight Velocity Can Support Frontline Health Workers in Predicting Malnutrition in HIV Exposed Infants: Preliminary Results from a Dream Cohort in Malawi. Minerva Pediatr. 2019 Mar 21. doi: 10.23736/S0026-4946.19.05417-3.
- Buonomo E, Scarcella P, Tembo D, Giuliano M, Moramarco S, Palombi L, et al. Malnutrition Decreases the Odds of Attaining Motor Milestones in HIV Exposed Children: Results from a Pediatric DREAM Cohort. Epidemiol Prev 2015; 39(4 Suppl 1):108-12.
- FAO. World Food Day 2018 Toolkit for Private Companies and Corporations. 16 October 2018. http://www.fao.org/3/CA0576EN/ca0576en.pdf
- Zambia Data Portal Central statistic office website. http://zambia.opendataforafrica.org/vzgcjrf/age-distribution
- Central Statistical Office (CSO) (Zambia), Ministry of Health (MOH) (Zambia), ICF International. Zambia Demographic and Health Survey 2013-14; Central Statistical Office, Ministry of Health, and ICF International: Rockville, MD, USA, 2014.